Coeliac disease is an autoimmune disorder that is triggered by gluten. It occurs in genetically predisposed individuals and leads to a lifelong enteropathy. It is thus not an allergy. The autoantigen in coeliac disease is the tissue transglutaminase of the small intestine in the complex with the gluten ingested through food. Since only HLA molecules DQ2, DQ7 or DQ8 can bind to gluten and present it to the immune system, only carriers of these HLA types are affected by the disease. With a prevalence of 1:200–1:500, the disease is not uncommon.
Most coeliac patients (99%) carry HLA types DQ2, DQ8 or DQ7. There is evidence that only HLA molecules can present gluten peptides. This means, for those who do not have one of the HLA types indicated, it is virtually impossible to develop coeliac disease. This makes the test for HLA-DQ2/DQ7/DQ8 very valuable for excluding coeliac disease.
Certain diseases, primarily autoimmune diseases, are very closely associated with coeliac disease. If they occur together, coeliac disease is often asymptomatic:
Pathophysiologically, coeliac disease is a T-cell-mediated inflammatory autoimmune process in genetically disposed individuals, which is directed against the small intestine tissue. Diagnostic tests thus include serological, genetic and histological investigations.
Serological laboratory tests are very important. Highly sensitive serological antibody tests not only allow the diagnosis of coeliac disease, but can also be used for follow-up. The following antibody tests are available:
Endomysial and transglutaminase IgA antibodies are very specific markers for the presence of coeliac disease and in the combination of these two assays ensure high sensitivity (~ 100%) and specificity (~ 100%) in the diagnosis of coeliac disease.
Please keep in mind:
Testing for HLA-DQ2, DQ7 and DQ8 as alleles responsible for celiac disease predisposition is primarily carried out to identify risk patients and for exclusion of coeliac disease. This is possible because these HLA characteristics are an essential prerequisite for coeliac disease (99% of celiac disease patients carry one of the above HLA characteristics). It is almost impossible for patients, who do not carry these HLA characteristics, to develop coeliac disease. The determination of the HLA is not influenced by any diet.
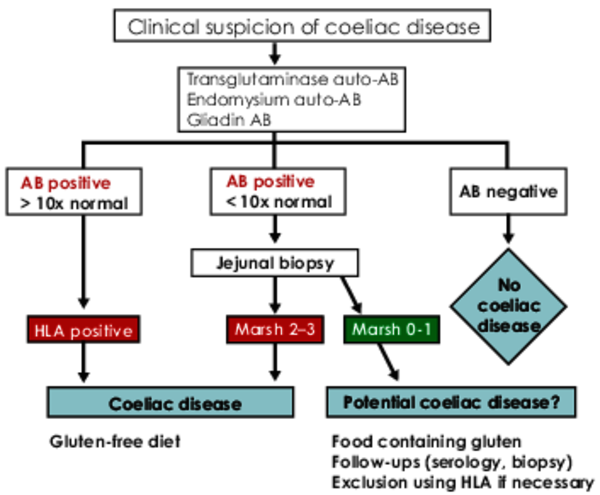
The realisation that coeliac disease is the disease closest associated with HLA, led to new ESPGHAN (European Society of Paediatric Gastroenterology, Hepatology and Nutrition) guidelines in 2012, and to new S2k guidelines of the German Society for Digestive and Metabolic Diseases in 2014. Both guidelines include the HLA test as a new diagnostic parameter. Regarding the recommended diagnostic algorithms, the guidelines distinguish between
What is new is that symptomatic patients with coeliac disease can now be tested for coeliac disease without the need for biopsy, as long as one of the HLA types DQ2/DQ7/DQ8 is present together with clinical symptoms and positive serology results.
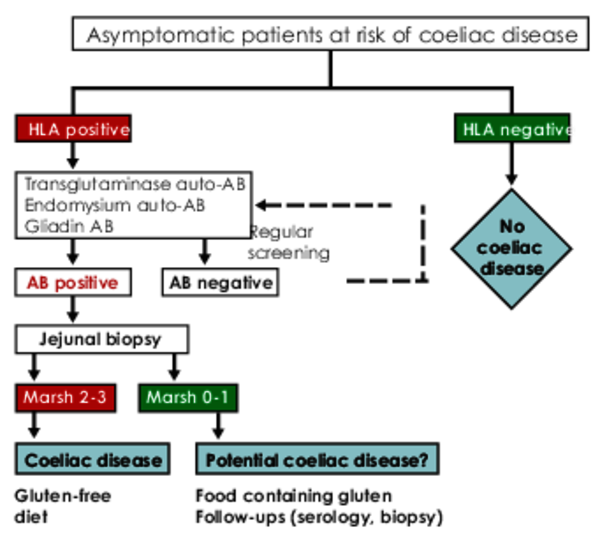
In patients with an increased risk of developing coeliac disease due to the diseases above and for first-degree relatives of coeliac sufferers, screening should start with the HLA determination. This means that regular screens for antibodies are no longer necessary with a negative HLA result. HLA-DQ2/7/8 positive individuals should be tested for TG2 IgA every two to three years.
Serology: 5 ml of serum
HLA-genotyping: 2 ml EDTA blood
Order: HLA with suspected coeliac disease. Please attach patient informed consent.
The costs for the test is 125,00 €.
Dr. Sabine Schütt